Happy National HIV Testing Day #stigmawarriors! Today we decided to present a timeline to show how far testing of HIV and AIDS has come in the United States, especially since there is a renewed effort by the LGBT community, HIV community, and the medical community to remove the stigma surrounding getting tested!
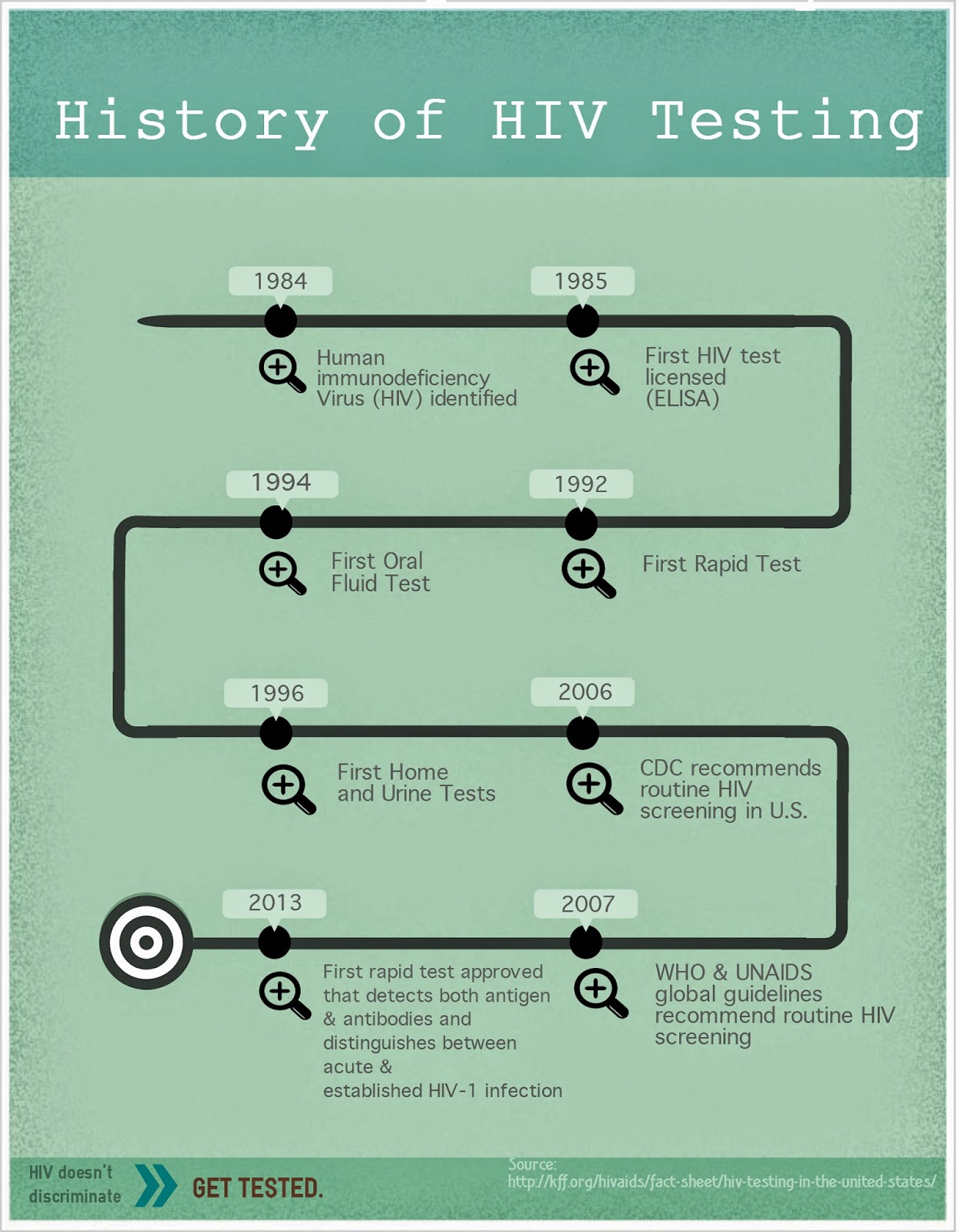
The history of HIV testing is almost as old as the history of HIV in the United States, and since the 1980s the types of tests and how they detect HIV have changed so much. Let's take a look at how far HIV testing has come!
The history of HIV testing is almost as old as the history of HIV in the United States, and since the 1980s the types of tests and how they detect HIV have changed so much. Let's take a look at how far HIV testing has come!
1980-1984:

- The City and County of San Francisco, working with the Shanti Project and the San Francisco AIDS Foundation, set up the San Francisco Model of Care in 1982, emphasizing home and community testing, care and treatment services [1].
- The following year, in May 1983, Congress passed the first bill that included funding specifically targeted at AIDS research, which lead to developments in testing and treatment [2].
1985-1989:
Between 1985, there was a lot of developments when it came to HIV testing!- The FDA licensed ELISA, the first commercial blood test which tested for HIV antibodies in the blood. Blood banks immediately began testing the US blood supply [3].
- Unfortunately, the Pentagon announced in the summer of 1985 that the military would immediately begin testing all new recruits for HIV infections, with the intention to reject anyone who tested positive. This policy sadly continues today [4].
- On December 6, 1985, the US Public Health Services issued the first recommendations for the prevention of mother-to-child transmission [5].
- In April 1987, the FDA approved the Western Blot Blood Test Kit, a more specific test for HIV antibodies [6].
- On August 14, 1987, the CDC issued the Perspectives in Disease Prevention and Health Promotion Public SafetyGuidelines for Counseling and Antibody Testing to Prevent HIV Infection and AIDS [7].
- On August 18, 1987, the FDA sanctioned the first human tests of a candidate vaccine to prevent HIV [8].
- At the end of 1987, the FDA published regulations which required all blood and plasma collected in the US to be screened for HIV [9].
- IN 1988, the FDA doubled its efforts to test the US blood and plasma supply, and by the end of the year 100% of the US blood supply had been tested for HIV antibodies [10].
- More importantly, the first World AIDS Day took place on December 1, 1988 [11].
- In 1989, the FDA licensed the first diagnostic kit to test for HIV antigens. Prior to this all HIV tests had only tested for antibodies [12].

1990-1994:
- The early 1990s brought more new HIV tests and health regulations to the public. The first HIV test to test for both HIV-1 and HIV-2 antibodies was licensed in 1990 [13], and that same year the CDC adopted the HIV-prevention counseling model, a “client-centered” approach that focuses on the patient rather than the disease [14].
- On May 27, 1992, the FDA licensed a 10-minute diagnostic test kit which can be used by health professionals to detect the presence of HIV-1 [15].
- The following year, the FDA published an interim rule on December 14th establishing a requirement for certain infectious disease testing, donor screening, and record keeping to help prevent the transmission of HIV and Hepatitis B and C through human tissue used in transplantation [16].
- Later that month, on December 23rd, the FDA approved the first non-blood based collection kit utilizing oral fluid for use in the detection of the antibody to HIV-1 [17].

1995-1999:
- The National Association of People Living with AIDS launched the first National HIV Testing Day on June 27, 1995 [18].
- That same year, the FDA recommended that blood establishments should implement donor screening for HIV-1 antigen using licensed test kits [19].
- 1996 brought some of the biggest and quickest advancement in HIV testing to date. Within four months the FDA approved the first at-home testing and collection kit, a viral load test, and the first HIV urine test [20].
- In 1998, the FDA approved Cambridge Biotech HIV-1, a HIV-1 (Western Blot) test with a new indication for urine specimen testing [21].
2000-2004:
- The first National HIV Vaccine Awareness Day was observed in 2001, and the CDC announced an HIV Prevention Strategic Plan to cut annual HIV infections in the US by half within five years that same year [22].
- The following year, 2002, marked an important development in HIV testing. On November 7, the FDA approved the first rapid HIV diagnostic test kit for use in the United States that provides results with 99.6% accuracy in as little as 20 minutes. Unlike other antibody tests for HIV, this blood test can be stored at room temperature, requires no specialized equipment, and may be used outside of traditional laboratory or clinical settings, allowing more widespread use of HIV testing [23].
- HIV testing became even more widespread on February 3, 2003, when the Department of Health and Human Services expanded availability of the rapid HIV test from the current 38,000 laboratories to more than 100,000 sites, including physician offices and HIV counseling centers [24].
- In 2004, the first rapid oral fluid test and the first rapid-body test for plasma which detects HIV-1 and HIV-2 were approved by the CDC [25].

2005-2009:
- The CDC officially recommended routine HIV screenings in US health care settings for people aged 13-64, and yearly screening for populations considered to be "at-risk" in 2006.
- The WHO and UNAIDS updated their global guidelines in 2007 to include that same recommendation [26].
- On December 30, 2008, the FDA approved the first nucleic acid test to detect the presence of two less common types of HIV, HIV-2 and HIV-1 Group O, in donated blood plasma and human tissue [27].
- The following year, in 2009, the FDA, CDC, and other federal agencies promoted National HIV Testing Day to increase awareness of the importance of HIV testing to help improve the health of those at risk for getting HIV and to prevent future infections [28].
2010-2014:
- In 2010, the CDC approved the first test which detects HIV antigens and antibodies [29].
- The first rapid oral fluid home test, Oraquick, was approved by the CDC in 2012 [30].
- And in 2013, the CDC approved the first rapid test that detects HIV antigens and antibodies, and distinguishes between acute and established HIV-1 infections [31].
What a trip! I learned so much about the history of HIV testing that I never knew before! I hope you did too!
It shows just how far HIV testing really has come from the early days. With new testing technology people can even test inside the comfort of their own homes. Now the next step is removing the stigma surrounding HIV testing, which several public campaigns are striving to do. But the campaigns won't be successful without you, #stigmawarriors! Let's get out there today and every other day to reduce the stigma surrounding HIV testing, through our words and actions. That way, more people will feel encouraged and supported in taking charge of their health!
We hope National HIV Testing Day inspires you to get out there and be the best #stigmawarrior you can be!